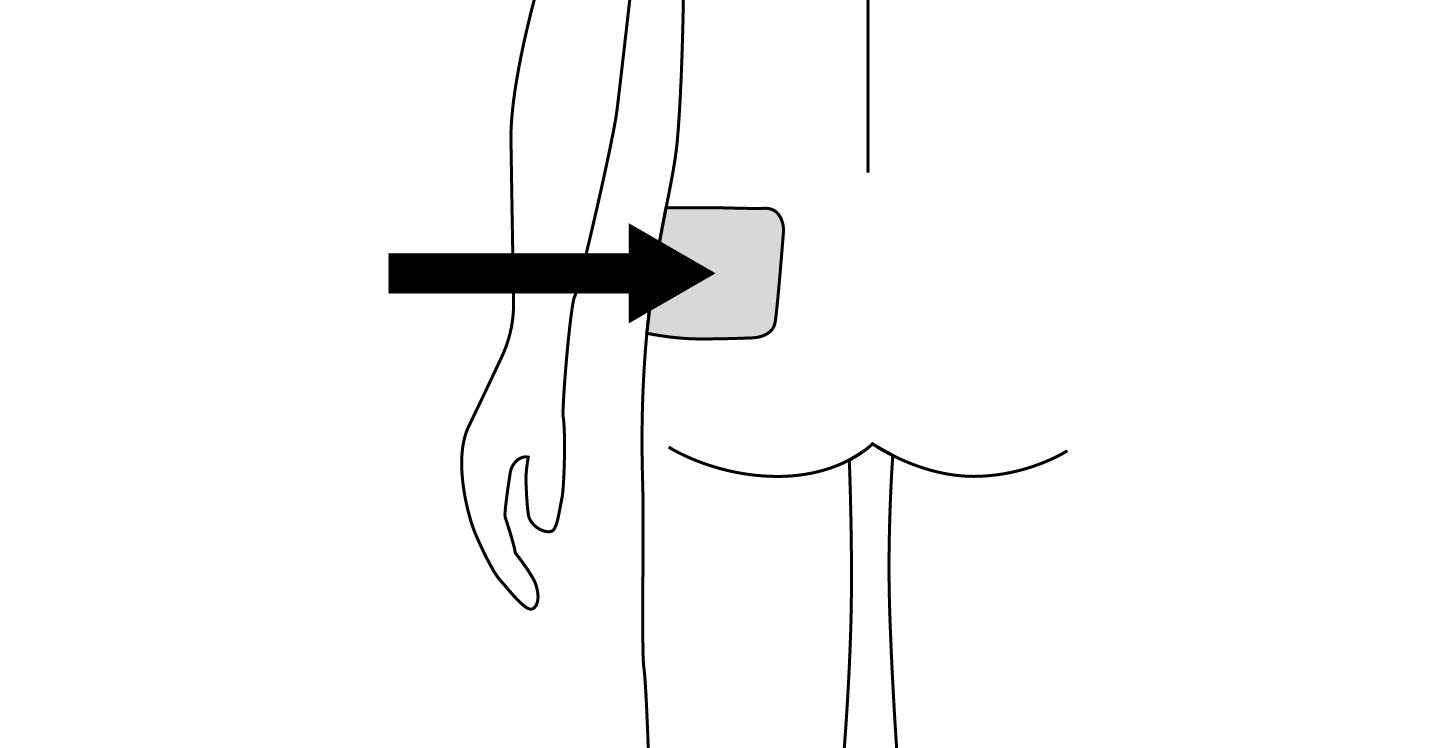
Following the initial dose, monthly doses can be administered in the gluteal or deltoid muscle.1

Following the initial dose, monthly doses can be administered in the gluteal or deltoid muscle.1
For patients who have never taken oral or injectable paliperidone, or oral or injectable risperidone: Establish tolerability with oral paliperidone or oral risperidone prior to initiating treatment with ERZOFRI®.
For schizophrenia
Monthly doses of 39 mg to 234 mg can be administered 4 weeks after first injection. The recommended monthly dose for schizophrenia is 117 mg.
For schizoaffective disorder
Monthly doses of 78 mg to 234 mg can be administered 4 weeks after first injection*
Support during the transition to ERZOFRI® and throughout treatment is available.
Learn more| Timing of missed dose | 4 to 6 weeks since last injection |
Dosing | Resume regular monthly dosing as soon as possible at the previously stabilized dose, followed by injections at monthly intervals |
| Timing of missed dose | >6 weeks to 6 months since last injection |
Dosing | Resume the same dose the patient was previously stabilized on (unless the patient was stabilized on a dose of 234 mg, then the first 2 injections should each be 156 mg) in the following manner:
|
| Timing of missed dose | >6 months since last injection |
Dosing | Restart dosing with recommended initiation:
|


When transitioning patients currently at steady-state on a long-acting injectable antipsychotic to ERZOFRI®:
Based on previous clinical response and tolerability, some patients may benefit from lower or higher doses within the available strengths (39 mg, 78 mg, 117 mg, 156 mg, and 234 mg):

Preparation and administration instructions
| To be prepared and administered by a healthcare professional only |
Read the instructions for preparation and administration below for preparation and administration considerations |
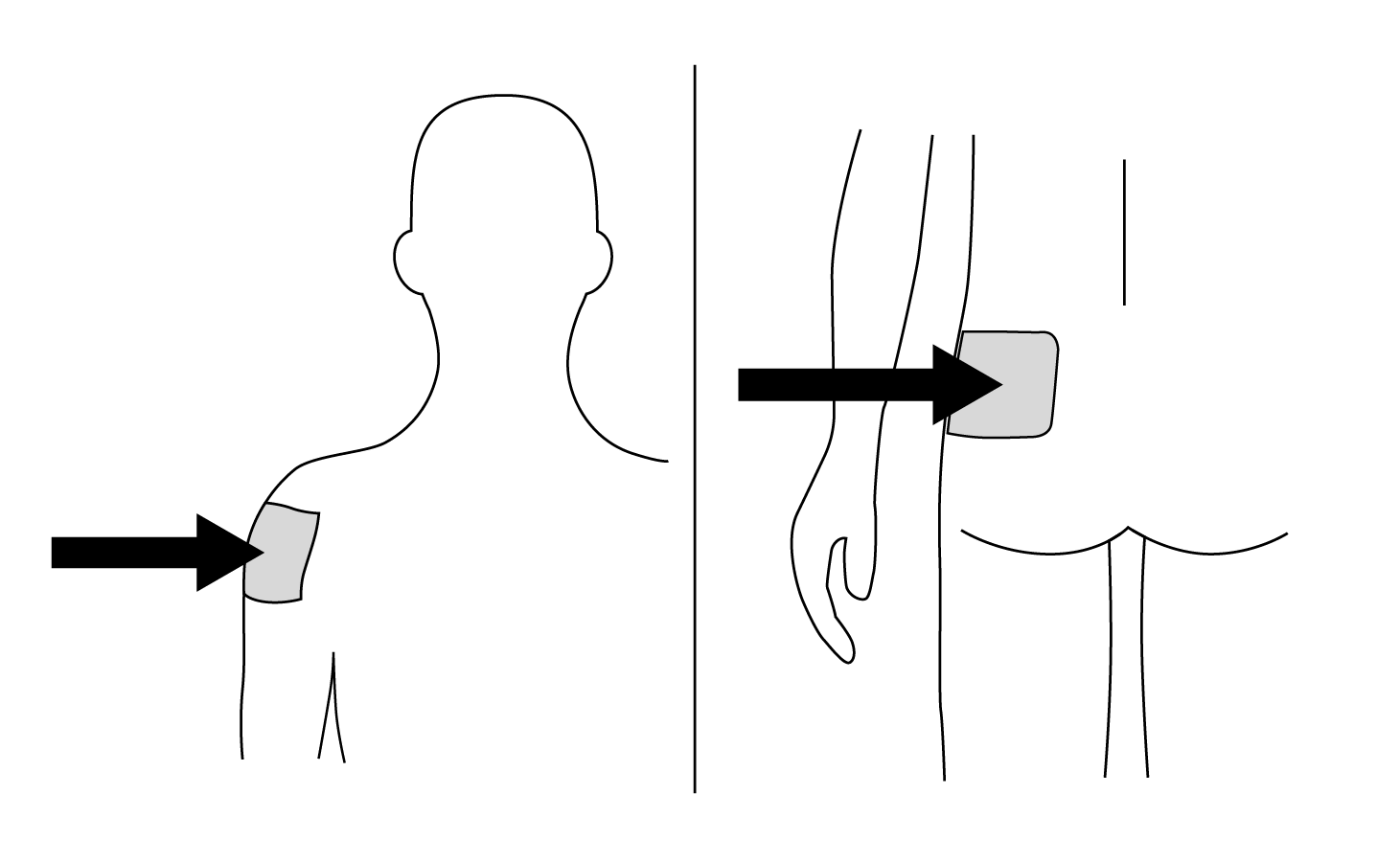
| For deltoid or gluteal intramuscular injection only |
Do not inject by any other route and, as a universal precaution, always wear gloves |
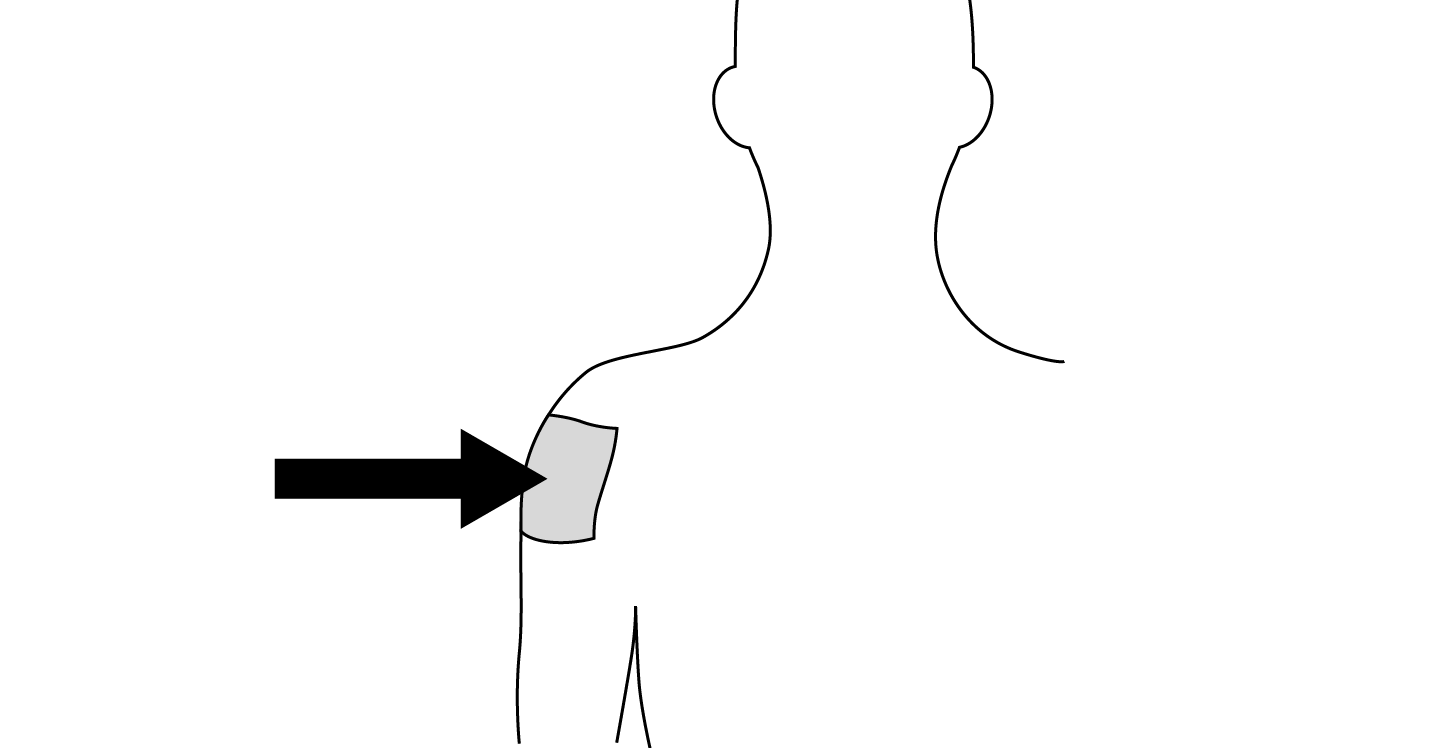
| Administer the initial dosage of ERZOFRI® in the deltoid muscle |
Subsequent monthly dosages may be administered in the deltoid or gluteal muscle |
| Do not substitute any component | The kit contains a prefilled syringe and 2 safety needles (a 1 ½-inch, 22-gauge needle and a 1-inch, 23-gauge needle) |
| Do not reuse | ERZOFRI® is for single use only |
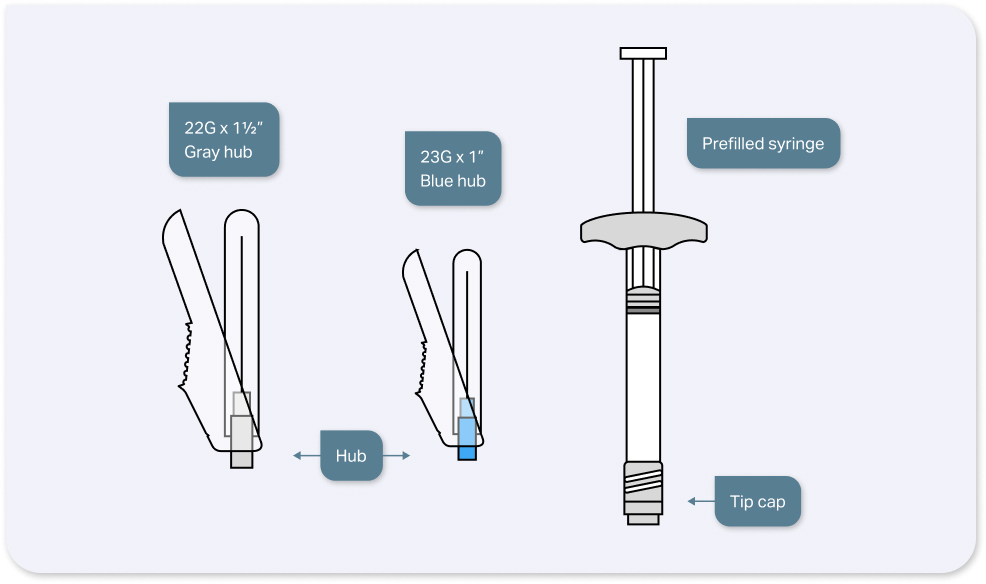
Step 1. Select needle1
If the patient weighs <90 kg, use the 1-inch, 23-gauge needle (needle with blue colored hub).
If the patient weighs ≥90 kg, use the 1 ½-inch, 22-gauge needle (needle with gray colored hub).
Use the 1 ½-inch, 22-gauge needle (needle with gray colored hub) regardless of patient’s weight.
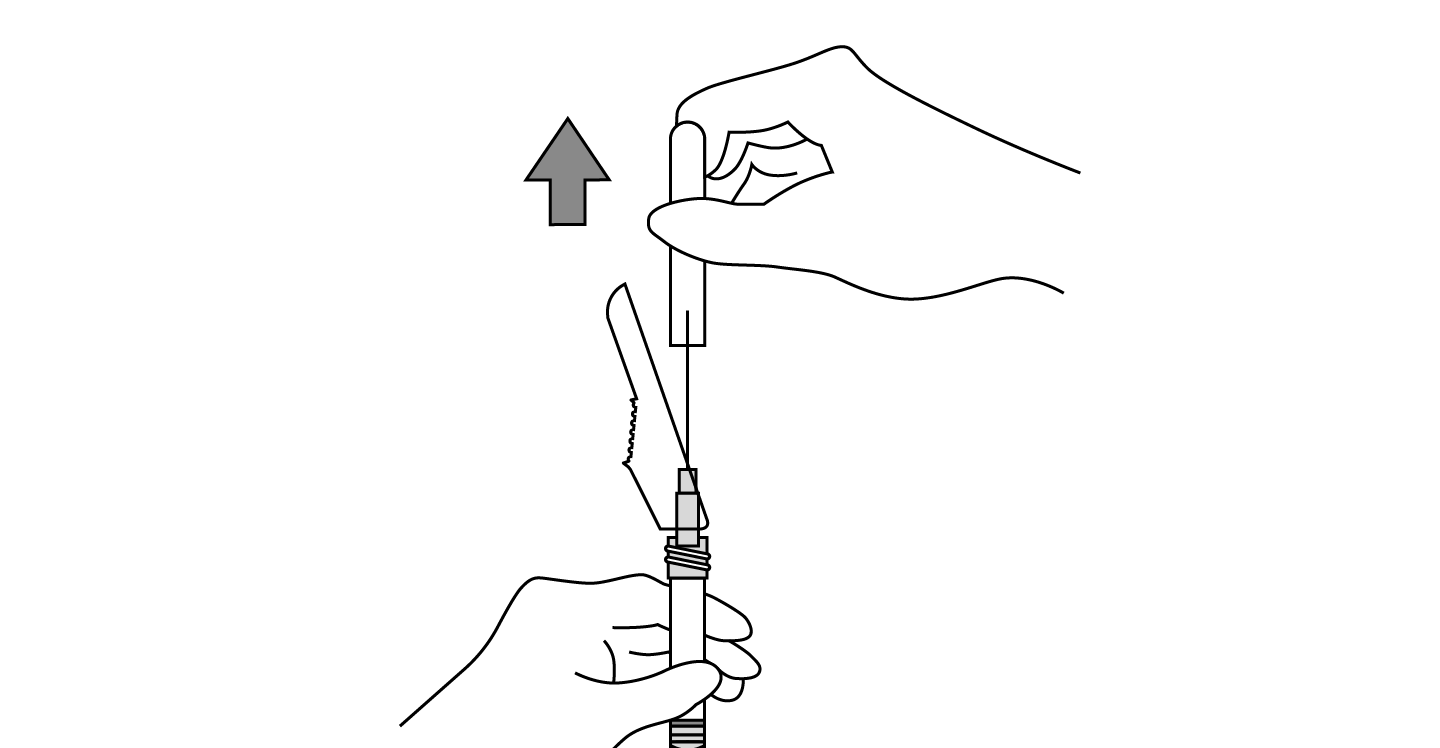
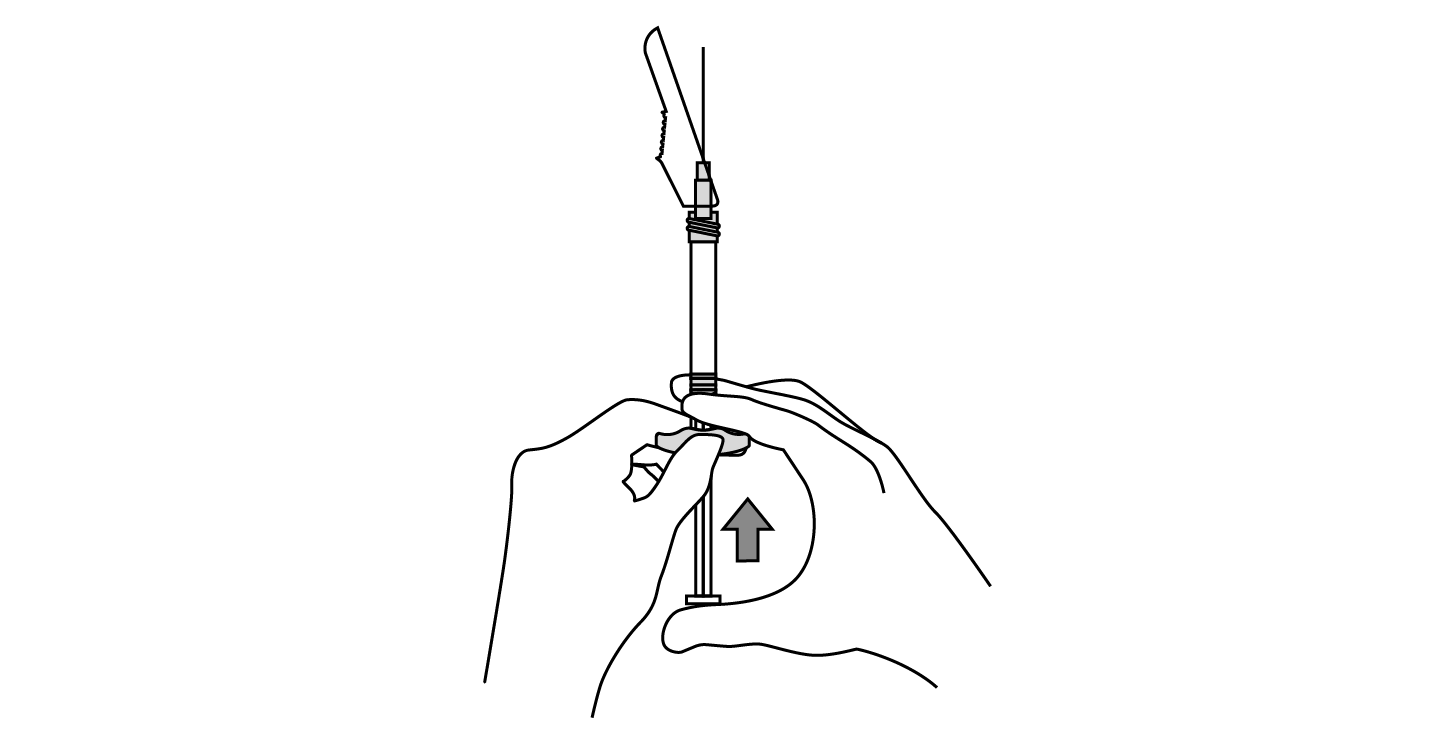
Step 2. Prepare for injection1
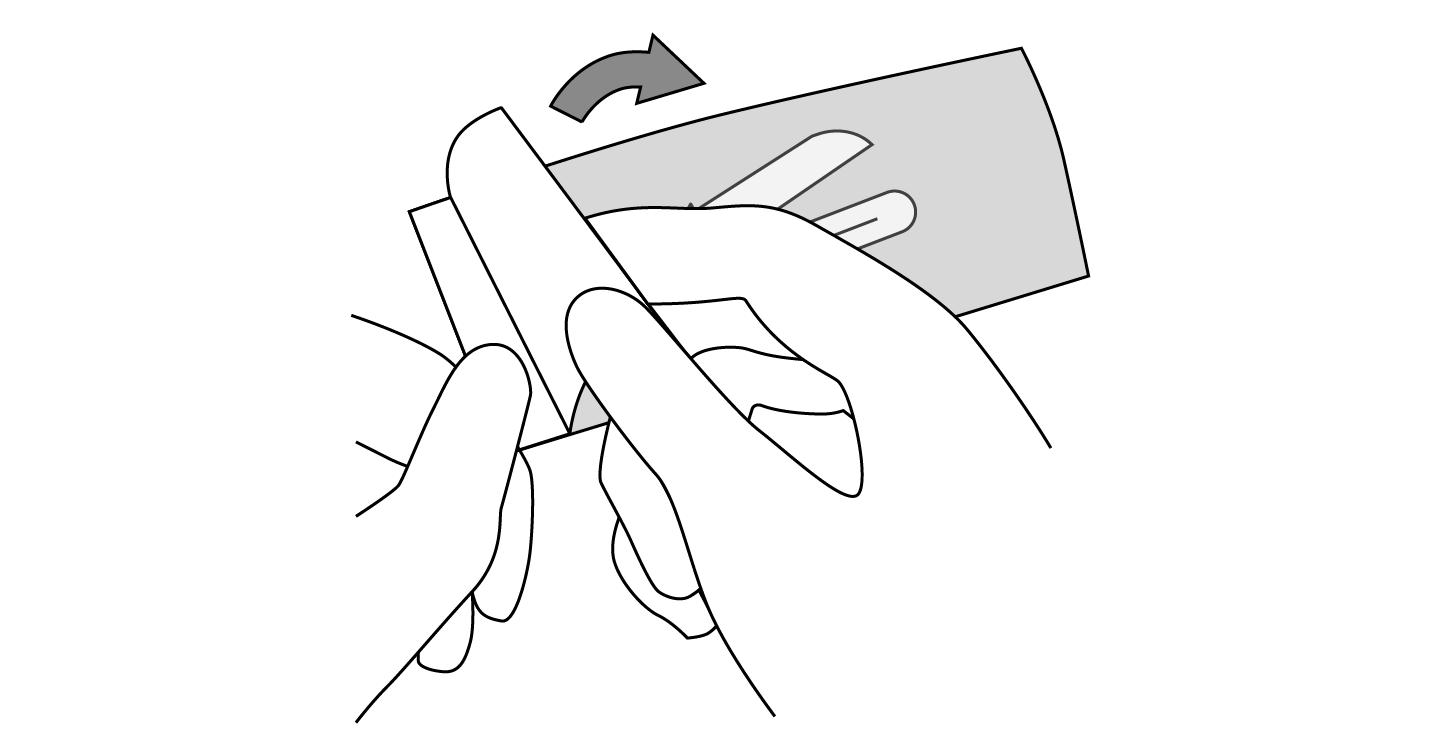
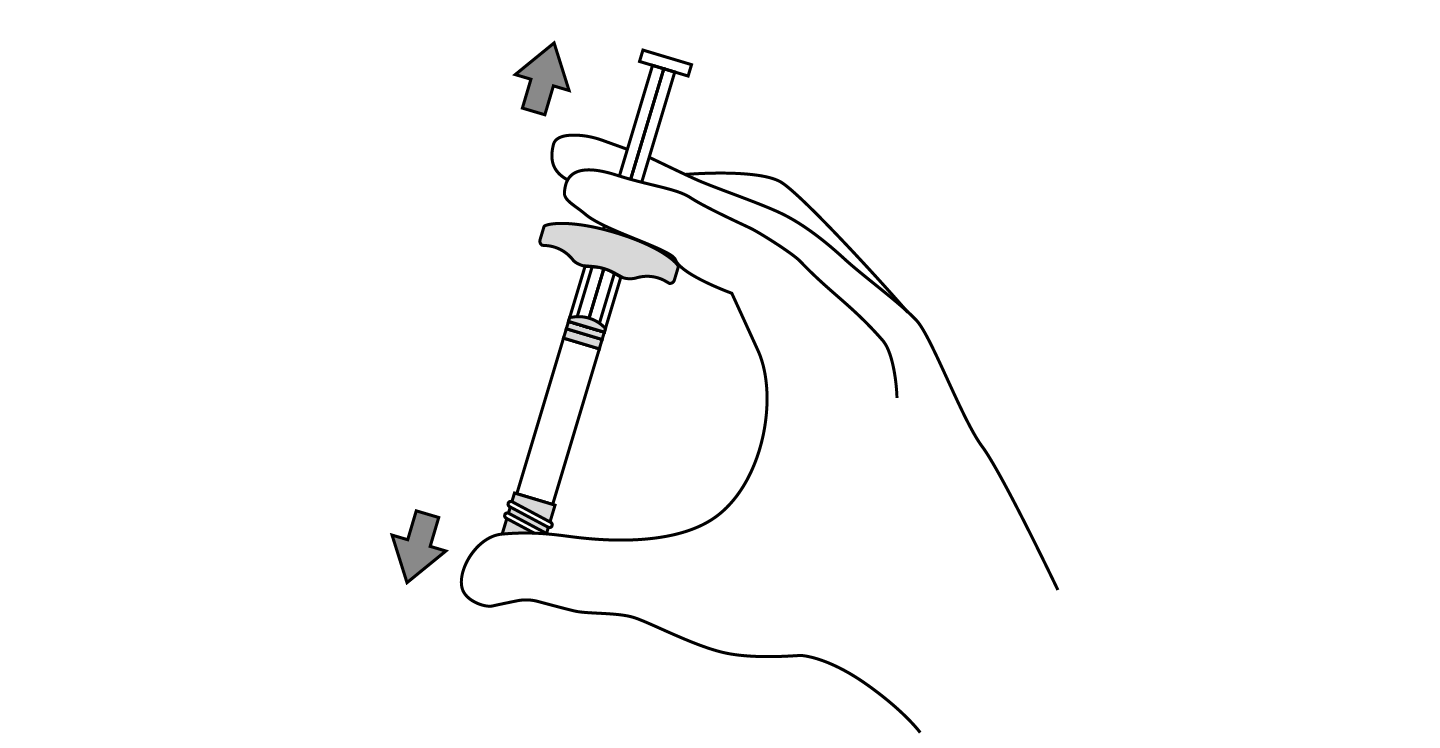
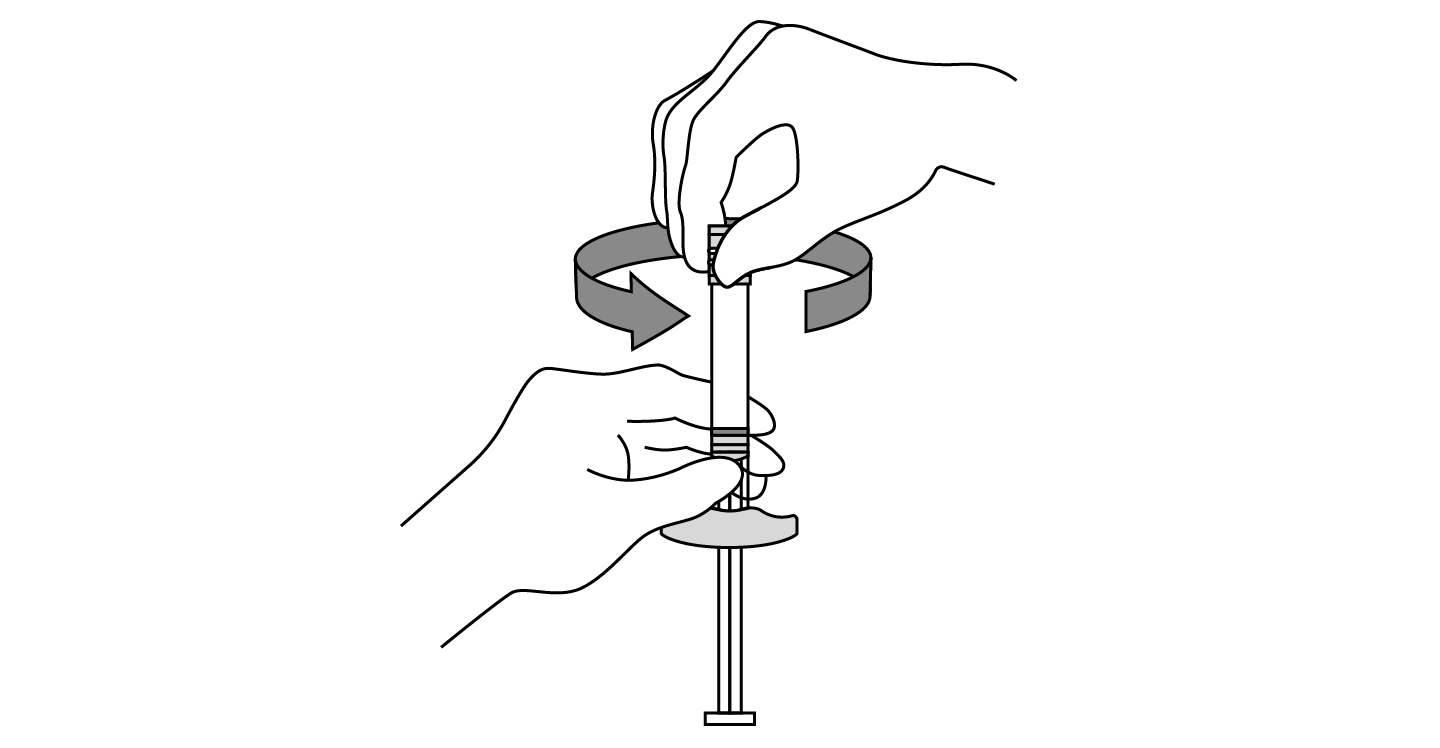
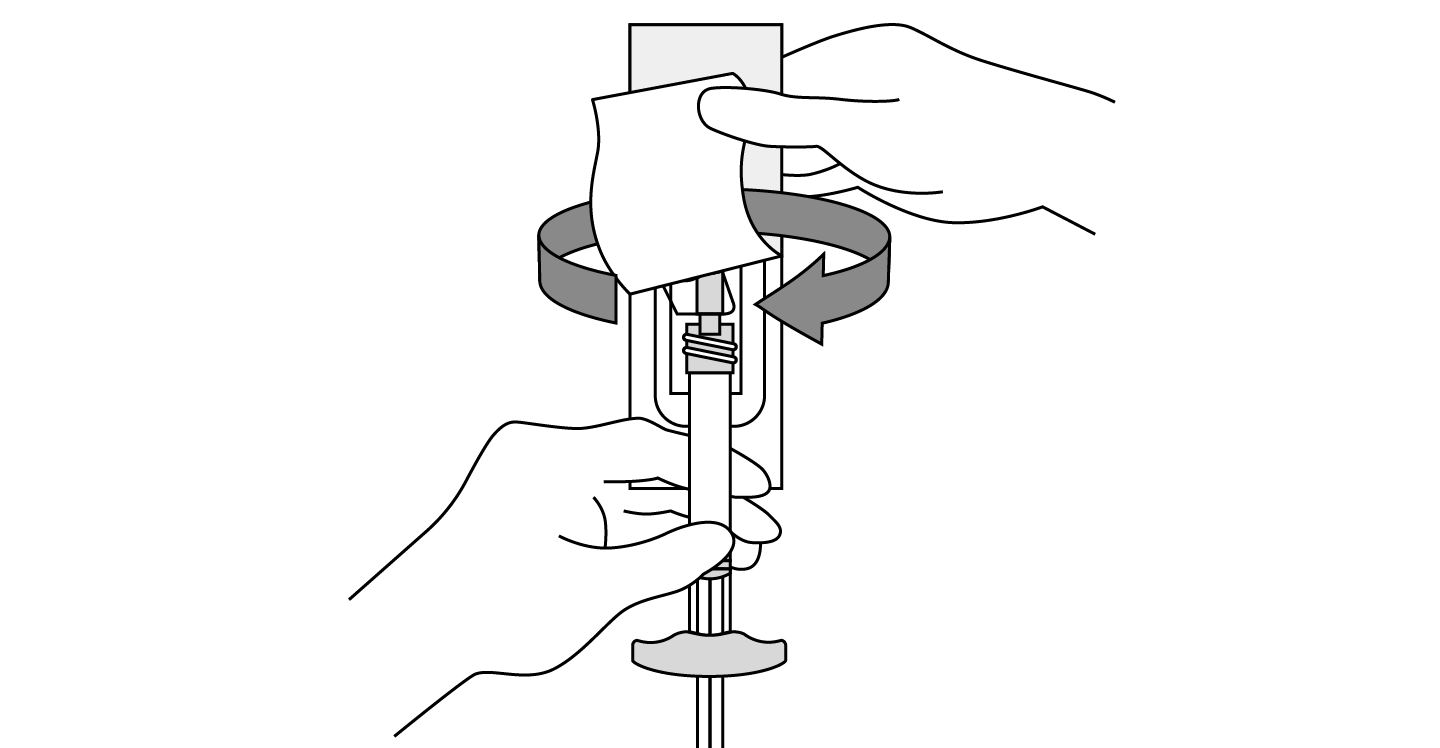
Do not remove the pouch until the syringe and needle are securely attached.
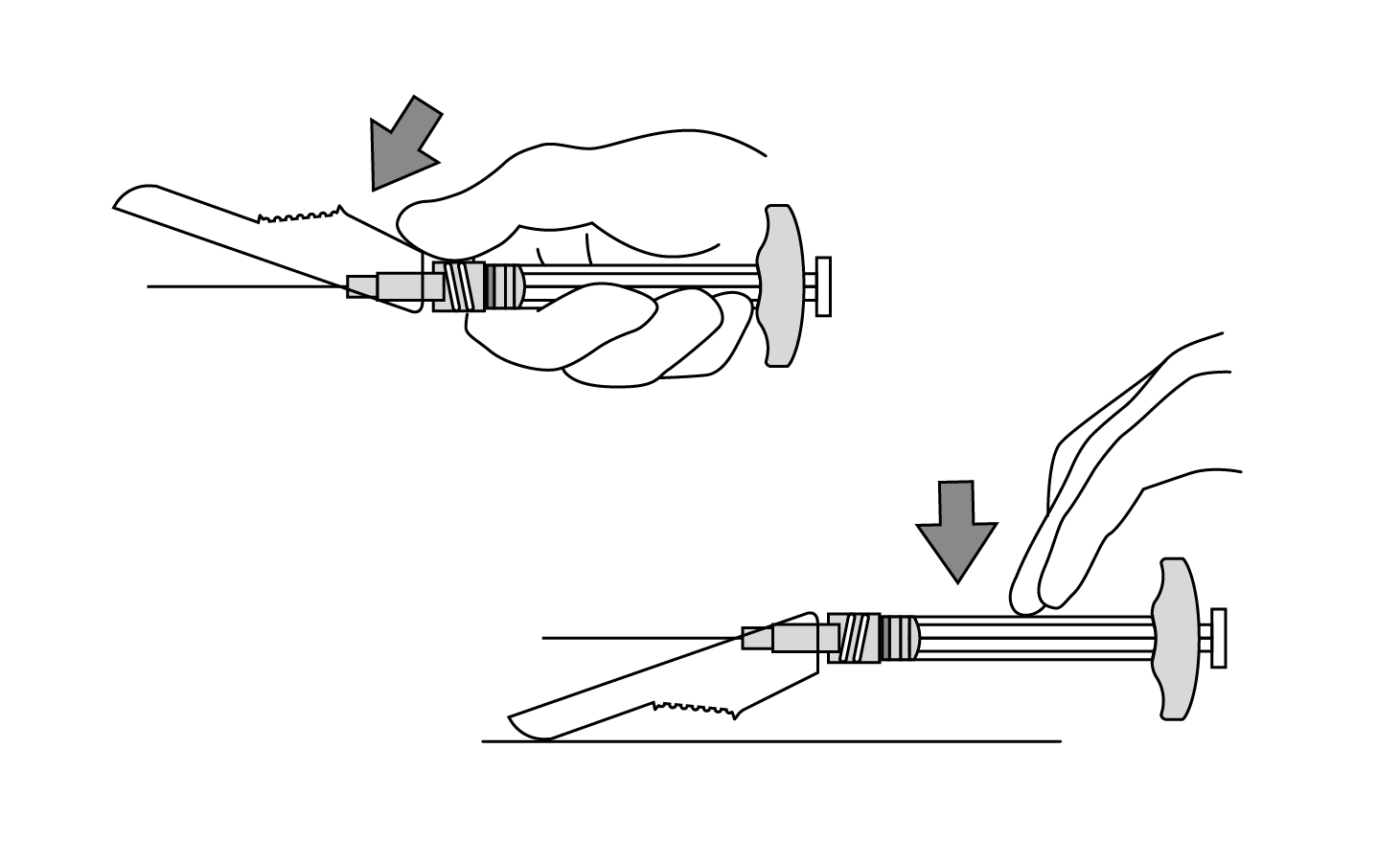
Step 3. Inject1
Step 4. After injection1

No refrigeration or warming are required in preparing or administering ERZOFRI®1


INDICATIONS AND USAGE: ERZOFRI® (paliperidone palmitate) extended-release injectable suspension for intramuscular use is an atypical antipsychotic indicated for the treatment of:
WARNING: INCREASED MORTALITY IN ELDERLY PATIENTS WITH DEMENTIA-RELATED PSYCHOSIS
Elderly patients with dementia-related psychosis treated with antipsychotic drugs are at an increased risk of death. ERZOFRI is not approved for use in patients with dementia-related psychosis.
ERZOFRI is contraindicated in patients with known hypersensitivity to paliperidone, risperidone, or to any excipients in ERZOFRI.
If signs and symptoms of TD appear in a patient treated with ERZOFRI, drug discontinuation should be considered. However, some patients may require treatment with ERZOFRI despite the presence of the syndrome.
The most common adverse reactions (incidence ≥5% and occurring at least twice as often as placebo) were injection site reactions, somnolence/sedation, dizziness, akathisia, and extrapyramidal disorder.
Pregnancy Exposure Registry: There is a pregnancy exposure registry that monitors pregnancy outcomes in women exposed to atypical antipsychotics, including ERZOFRI, during pregnancy. Healthcare providers are encouraged to register patients by contacting the National Pregnancy Registry for Atypical Antipsychotics at 1-866-961-2388 or online at http://womensmentalhealth.org/clinicaland-research-programs/pregnancyregistry/.
Risk Summary: Neonates exposed to antipsychotic drugs during the third trimester of pregnancy are at risk for extrapyramidal and/or withdrawal symptoms following delivery. Overall, available data from published epidemiologic studies of pregnant women exposed to paliperidone have not established a drug-associated risk for major birth defects, miscarriage, or adverse maternal or fetal outcomes. There are risks to the mother associated with untreated schizophrenia and with exposure to antipsychotics, including ERZOFRI, during pregnancy.
Lactation: Infants exposed to ERZOFRI through breastmilk should be monitored for excess sedation, failure to thrive, jitteriness, and extrapyramidal symptoms (tremors and abnormal muscle movements).
Fertility: Treatment with ERZOFRI may result in an increase in serum prolactin levels, which may lead to a reversible reduction in fertility in females of reproductive potential.
Renal Impairment: Use of ERZOFRI is not recommended in patients with moderate or severe renal impairment (creatinine clearance <50 mL/min).
Patients with Parkinson’s Disease or Lewy Body Dementia: Patients with Parkinson’s Disease or Dementia with Lewy Bodies can experience increased sensitivity to ERZOFRI. Manifestations can include confusion, obtundation, postural instability with frequent falls, extrapyramidal symptoms, and clinical features consistent with neuroleptic malignant syndrome.
Please see full Prescribing Information for ERZOFRI® including BOXED WARNING.



